In Part I of this article, I talked about some of the outdated—and sometimes even dangerous—approaches to diagnosing and treating prostate cancer. In this concluding part, we’ll learn about some new-, safer-, and more-effective technologies doctors are using to diagnose and treat the number one cancer in men.
 Perhaps one of the most important of these new technologies is an advanced prostate MRI, also known as a multiparametric MRI. For the first time, we can see into the prostate gland and differentiate cancerous tissue from normal prostate tissue. My MRI showed that I had cancer in only one area, the left lobe. It was located in a very safe area, far from any important structures and showing no sign of spread out of the gland. I asked myself, why undergo radical treatment that would remove or burn the entire prostate gland with its high risk of side effects when the low-grade cancer existed in only one limited area?
Perhaps one of the most important of these new technologies is an advanced prostate MRI, also known as a multiparametric MRI. For the first time, we can see into the prostate gland and differentiate cancerous tissue from normal prostate tissue. My MRI showed that I had cancer in only one area, the left lobe. It was located in a very safe area, far from any important structures and showing no sign of spread out of the gland. I asked myself, why undergo radical treatment that would remove or burn the entire prostate gland with its high risk of side effects when the low-grade cancer existed in only one limited area?
Each of the surgeons had told me that if a man has prostate cancer in one area, he very likely has it in many other areas. Thus the rationale for treating the entire gland. But my MRI showed that my cancer only existed in one area. At the same time, a newly published study from the Cleveland Clinic countered the surgeons’ view. Of 179 men who had unilateral prostate cancer and chose prostatectomy, only 29% significant cancer elsewhere in the gland. 71% either had unilateral disease or tiny, insignificant cancers on the opposite side. These 71% hadn’t needed prostatectomy!
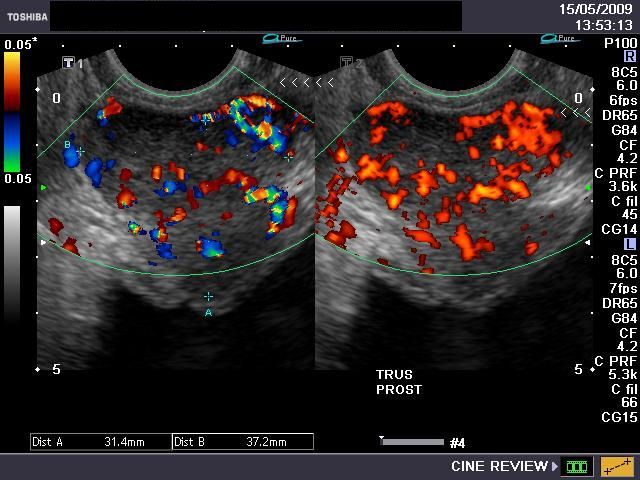 One question remained: should I treat my prostate cancer or wait? “Watchful Waiting,” the old do-nothing approach did not appeal. Yet its newer model, “Active Surveillance,” which encompasses regular PSA tests, MRI and another imaging method, Color Doppler Ultrasound, made more sense. With a low-grade, Gleason 6 cancer, the odds were good that it would never be a threat. And if it changed, the odds were good we’d catch it early.
One question remained: should I treat my prostate cancer or wait? “Watchful Waiting,” the old do-nothing approach did not appeal. Yet its newer model, “Active Surveillance,” which encompasses regular PSA tests, MRI and another imaging method, Color Doppler Ultrasound, made more sense. With a low-grade, Gleason 6 cancer, the odds were good that it would never be a threat. And if it changed, the odds were good we’d catch it early.
I had other choices too. High Intensity Focused Ultrasound (HIFU), a burning technique, and cryosurgery, a freezing technique, can be applied to half of the prostate gland or to a localized area. These procedures can be done in a few hours in an outpatient surgical center. Adverse effects occur but far less often than with the radical approaches.
Another interesting technique is now appearing on the horizon. Focused Laser Ablation (FLA) is now being studied for use for localized prostate cancer and available to the public. FLA is designed specifically for focal treatment. It too takes a few hours. Early reports are encouraging.
Each of these three techniques is performed under MRI guidance, thereby greatly improving accuracy. Indeed, the image of the cancerous tissue can be seen to die as these treatments are applied.
It will be many years before the new diagnostic tests and methods for focal treatment are widely available. Studies demonstrating their reliability need to be replicated. Medical associations will have to review the study results and vote to approve. This takes time. Out of caution, the medical system moves slowly, and sometimes too slowly.
I wrote Prostate Cancer Breakthroughs to help spread the word. After my close call with overtreatment, men need to know there are more options than the outdated all-or-nothing approach to treating prostate cancer.